| 5-Amino 1MQ | NNMT inhibitor (small molecule) | Metabolic, Longevity | ORAL | Subject to evolving FDA review |  |
| AOD-9604 | GH C-terminal fragment | GH axis, Metabolic | INJ | Subject to evolving FDA review |  |
| BPC-157 | Pentadecapeptide (research peptide) | Recovery | INJ | Subject to evolving FDA review |  |
| Bremelanotide / PT-141 | Melanocortin receptor agonist | Sexual health | INJ | Available with valid Rx |  |
| CJC-1295 | GHRH analog (long-acting peptide) | GH axis | INJ | Subject to evolving FDA review |  |
| Compounded Semaglutide | GLP-1 receptor agonist | Metabolic | INJ | Valid patient-specific Rx required |  |
| Compounded Tirzepatide | Dual GIP/GLP-1 receptor agonist | Metabolic | INJ | Valid patient-specific Rx required |  |
| DSIP, Delta Sleep-Inducing Peptide | Sleep-related nonapeptide | Sleep | INJ | Subject to evolving FDA review |  |
| Epitalon / Epithalon | Pineal tetrapeptide | Longevity, Sleep | INJ | Subject to evolving FDA review |  |
| GHRP-2 / GHRP-6 | GH-releasing peptide | GH axis | INJ | Subject to evolving FDA review | 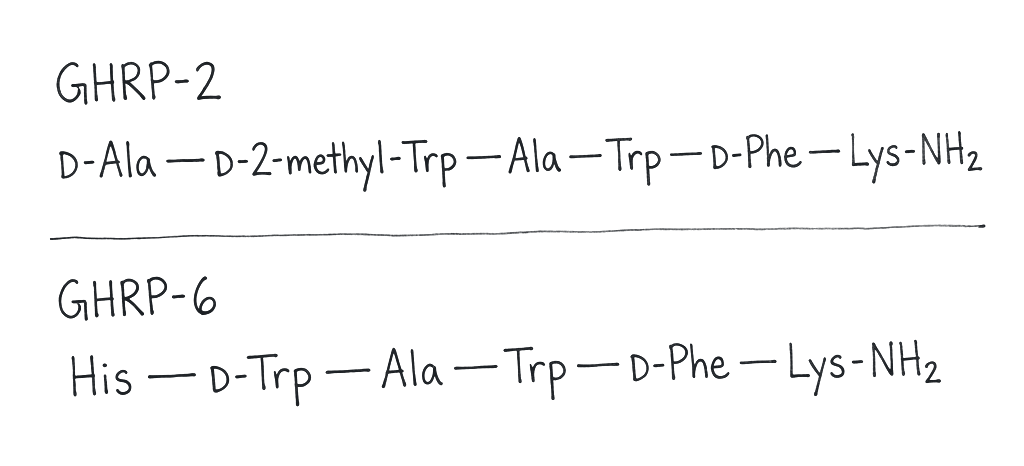 |
| Hexarelin | GH-secretagogue hexapeptide | GH axis | INJ | Subject to evolving FDA review | 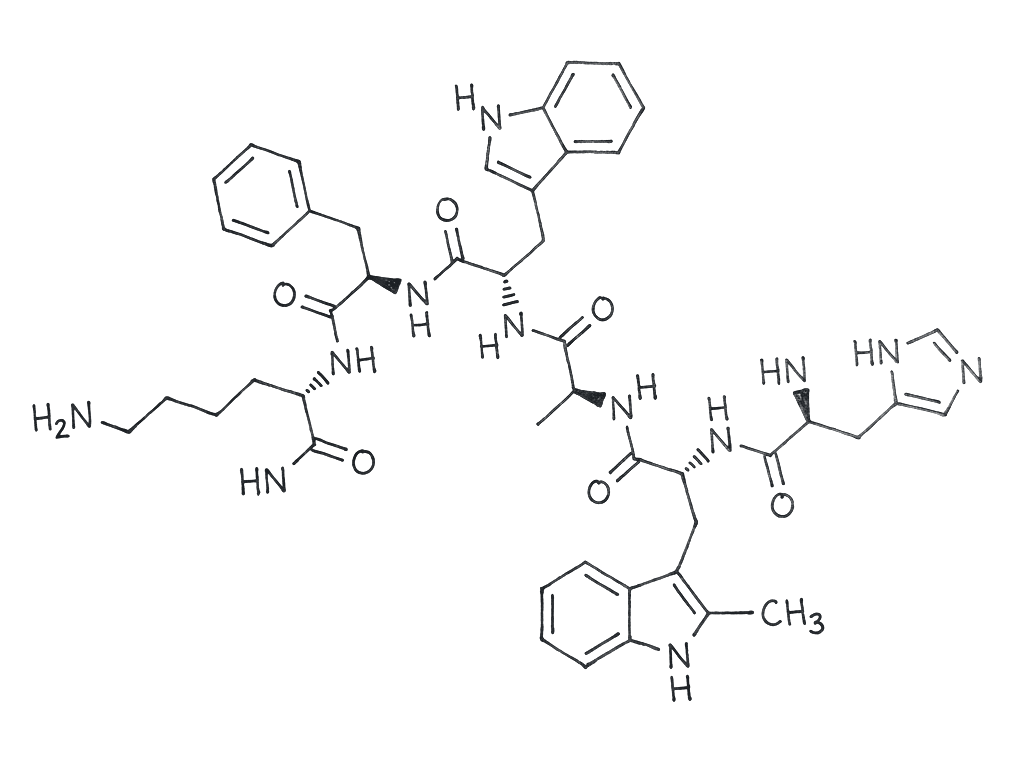 |
| Ipamorelin | Selective ghrelin receptor agonist (peptide) | GH axis | INJ | Subject to evolving FDA review | 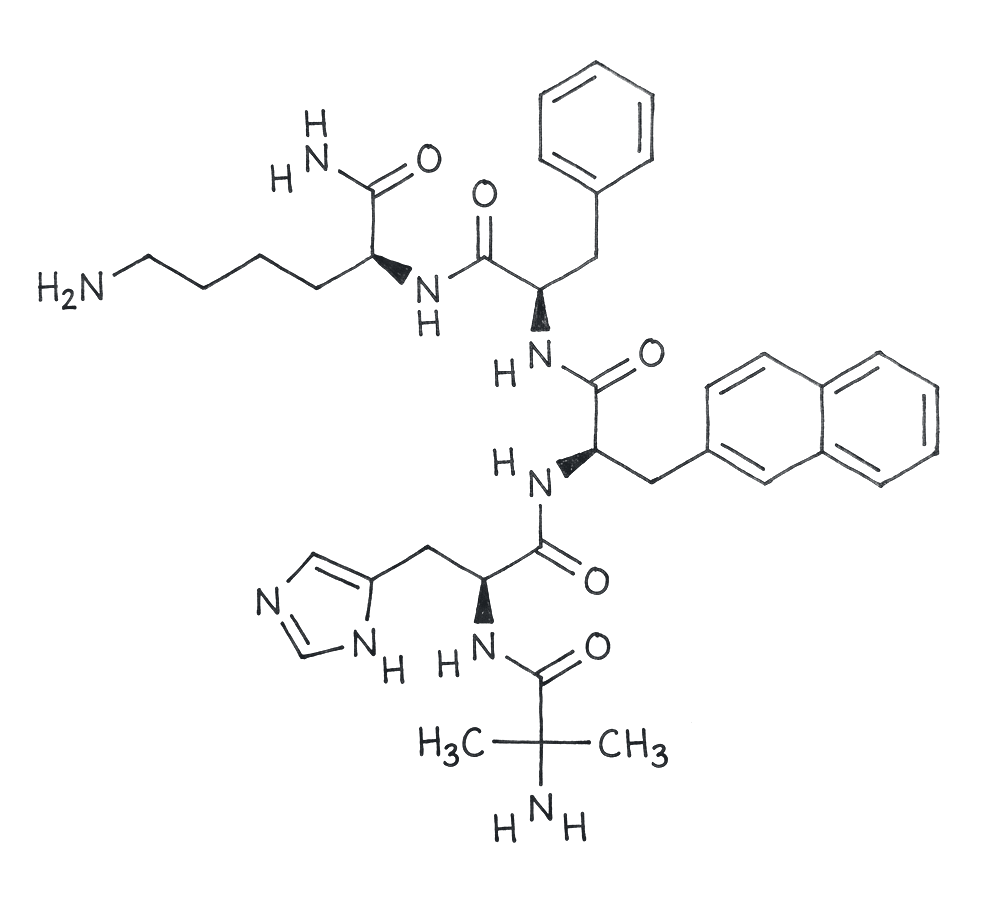 |
| KPV | Tripeptide (α-MSH fragment) | Recovery, Skin | TOPICAL · INJ · ORAL | Subject to evolving FDA review |  |
| LL-37 | Cathelicidin antimicrobial peptide | Immune | INJ · TOPICAL | Subject to evolving FDA review |  |
| MK-677 / Ibutamoren | Orally active GH secretagogue (small molecule) | GH axis | ORAL | Subject to evolving FDA review |  |
| MOTS-C | Mitochondrial-encoded peptide | Metabolic | INJ | Subject to evolving FDA review |  |
| Pentadeca Arginate (PDA) | Pentadecapeptide arginate | Recovery | INJ · ORAL | Subject to evolving FDA review |  |
| Selank | Tuftsin-derived heptapeptide | Cognition | INJ · TOPICAL | Subject to evolving FDA review |  |
| Semax | ACTH-derived peptide | Cognition | INJ · TOPICAL | Subject to evolving FDA review |  |
| Sermorelin | GHRH analog (peptide) | GH axis, Longevity | INJ | Valid patient-specific Rx required |  |
| TB-500 / Thymosin Beta-4 | Thymosin beta-4 peptide fragment | Recovery | INJ | Subject to evolving FDA review |  |
| Tesamorelin | GHRH analog (peptide) | GH axis | INJ | Valid patient-specific Rx required |  |
| Thymosin Alpha-1 / Thymalin | Thymic peptide (immunomodulatory) | Immune, Longevity | INJ | Subject to evolving FDA review |  |
| Vasoactive Intestinal Peptide (VIP) | Endogenous neuropeptide | Sleep | INJ | Subject to evolving FDA review |  |
